Our lead asset, bezisterim (NE3107), is a novel, orally administered small molecule that is both anti-inflammatory and insulin-sensitizing, and is currently being studied in Alzheimer’s disease, Parkinson’s disease and Long COVID. As part of the clinical trials in these core indications, we’re also exploring bezisterim’s potential impact on longevity by measuring its ability to reduce DNA methylation in study participants.
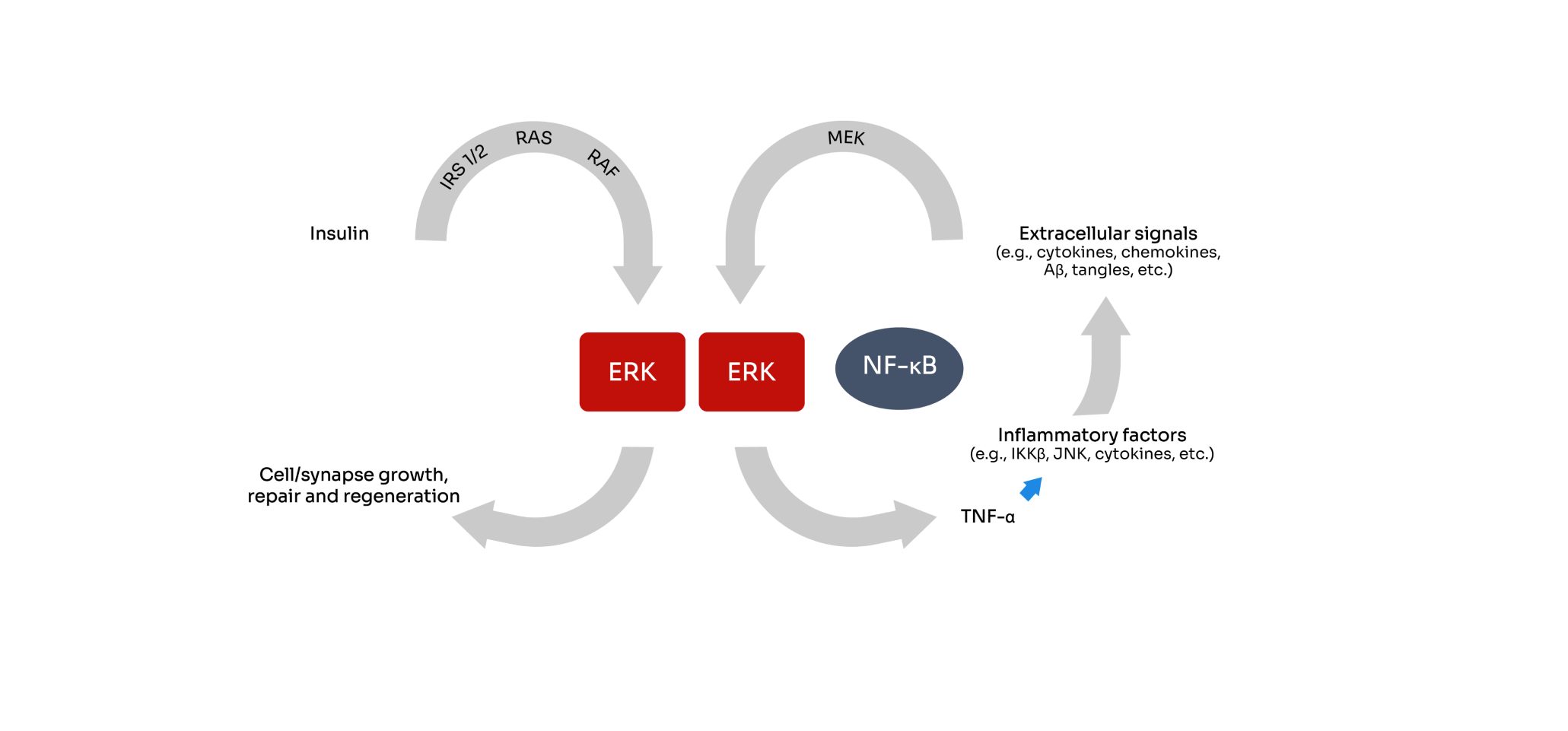
Bezisterim is an oral small molecule, blood-brain barrier (BBB) permeable, anti-inflammatory insulin sensitizer that binds extracellular signal-regulated kinase. Bezisterim has been shown to selectively inhibit inflammation-driven ERK- and NF-κB-stimulated inflammatory mediators, including tumor necrosis factor alpha (TNF-α), without inhibiting their homeostatic functions.
An extensive body of evidence shows that both inflammation and insulin signaling are central to the pathophysiology or symptom development of an increasing number of conditions.
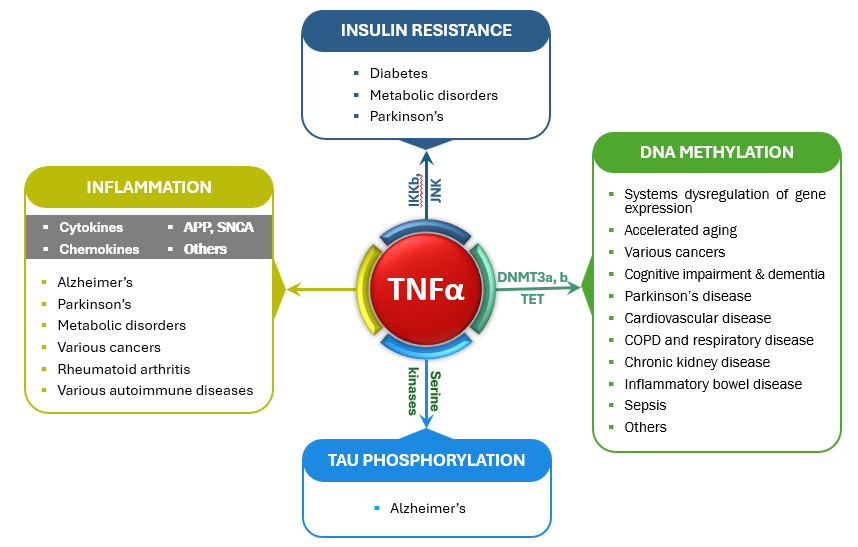
We believe TNFα-mediated chronic low-grade inflammation is the starting point for many things going wrong in the body. Chronic overproduction of TNFα has been shown to: